
Colonic Polyps – Current Understanding, Implications, Endoscopic approach & Surveillance
Written by


Background on Colonic polyps
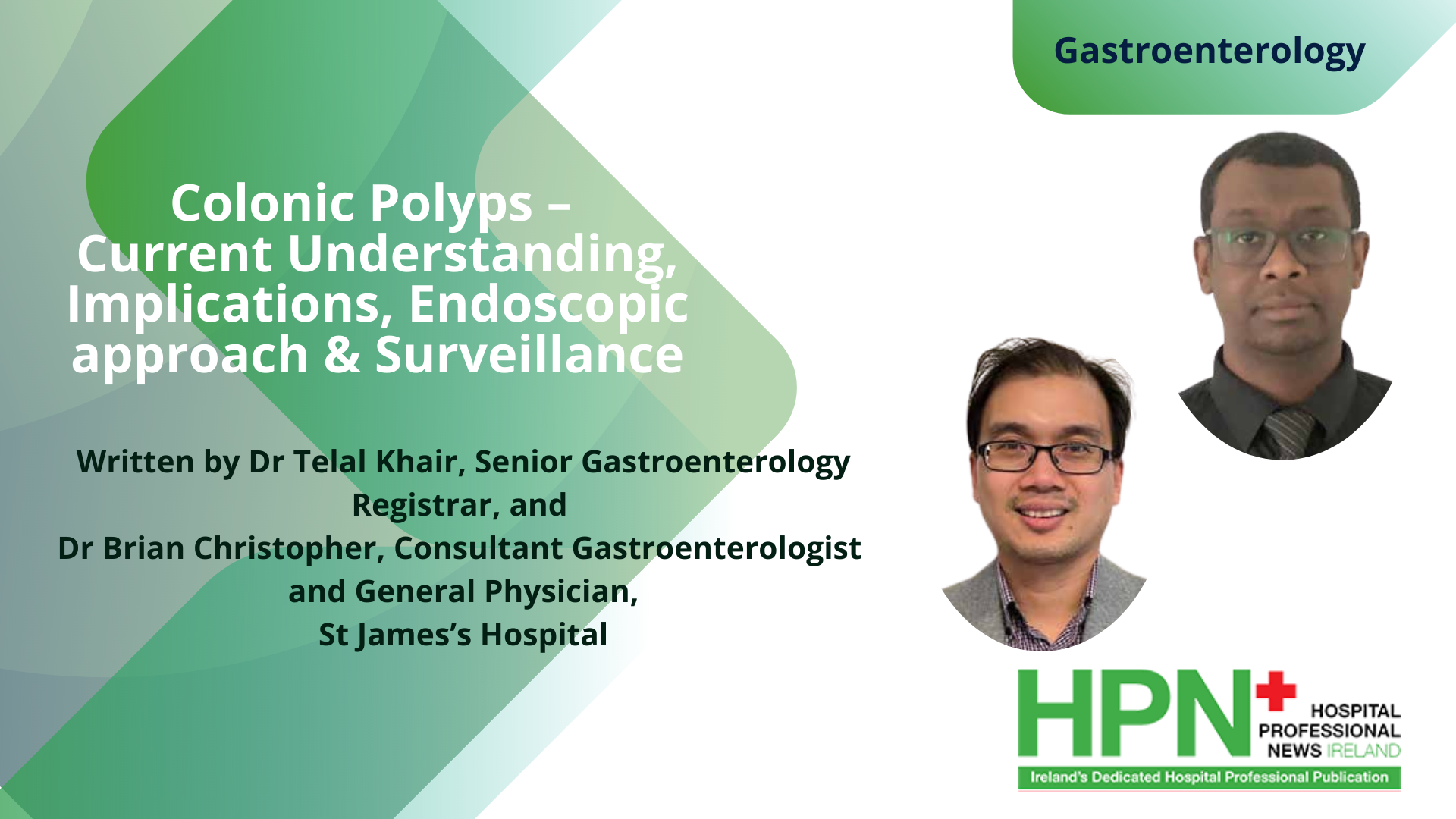
Colonic polyps (Image 1) are common finding at colonoscopy. There are different polyps aetiologies including hyperplastic, inflammatory, part of polyposis syndromes, pre-malignant and neoplastic. The endoscopic removal of colorectal polyps reduces the incidence of colorectal cancer (CRC) and is considered an essential skill for all endoscopists who perform colonoscopy 1,2,3 . Therapeutic polypectomy is a specialised procedure with timely intense training for trainees. Complex cases will need to be performed by expert endoscopists at tertiary centres and may need multi-disciplinary meeting discussion with fellow endoscopists and colorectal colleagues prior to intervention.
Diagnostic and therapeutic colonoscopic procedures totally gives a different perspective approach for any endoscopist and all cases are individualised. Proper consent with risk and benefit involved with the diagnostic procedure itself and the possibility of intervention should always be discussed with the patient preprocedure. Multifactorial aspects including co-morbidities, being on antiplatelets / anticoagulations factor, presence of pacemaker or Implantable Cardioverterdefibrillators (ICD), potential complications, aftermath of the procedure i.e. endoscopist’s impression of total complete polypectomy with histological confirmation (i.e. R0 resection margin), Gastro Histopathology multidisciplinary team discussion, surveillance pathway and so on must all be taken into account.
As with any other medical specialities, there are specific societies guideline committee that review and revise all the up to date, evidence-based approach and management of colonic polyps. These would include the European Society of Gastrointestinal Endoscopy (ESGE), British Society of Gastroenterology (BSG), American Society of Gastrointestinal Endoscopy (ASGE), United European Gastroenterology (UEG) and not forgetting our own, Irish Society of Gastroenterology (ISG) to name a few.
Please note that this article section is not intended to cover the entire all need to know about colonic polyps as the topic is too wide to be fully discussed here. Important sections are discussed in this article and ultimately, Gastroenterology service involvement with follow up on the appropriate future management going forward especially with regards to surveillance and appropriateness is warranted.
Endoscopy
At mentioned, preparation and anticipation is the key in endoscopy. Indications for being on anti-platelets or anticoagulation for patients undergoing colonoscopy should always be reviewed as findings at endoscopy will totally change the ball game approach altogether from diagnostic to therapeutic intervention. These should all be reviewed even at the colonoscopy referral phase with the appropriates to hold these medications beforehand and whether any interim intervention is indicated i.e. anticoagulation bridging, switching to aspirin etc. or even discussion with specific relevant specialties i.e. cardiology / haematology colleagues.

Good High Quality Colonoscopy
A good quality colonic mucosal view after standard bowel preparation is crucial as endoscopists must be able to have definite clear views of the entire colon including the key landmarks.
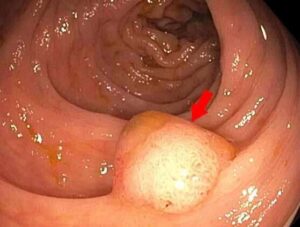
Standard position change during procedure should always be undertaken to optimize the yield of polyps’ detection. The use of other polyp detection enhancing methods i.e. computerised artificial intelligence (AI), endocuffs etc. (Image 2) are all depending on the availability in the local endoscopy department unit.
Endocuff is a device attached to the distal end of a colonoscope, designed to maintain and maximize the mucosa view during colonoscopy by manipulating colonic folds. A single row of flexible arms everts and flatten folds to provide an enhanced view of the entire colon and increase polyp and adenoma detection rate 4 .


Antiplatelet / Anticoagulation Guidelines
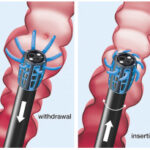
The current BSG / ESGE guidelines (2021) development committee included representatives from British Society of Haematology, British Cardiovascular Intervention Society and representatives from the charities Anticoagulation UK and Thrombosis UK 5
Endoscopic Classifications
Gross endoscopic morphology of polyps should be described using the Paris classification system and sized in milimeters 6 (moderate quality evidence; strong recommendation). Any polyps should be thoroughly inspected with the standard endoscopy white light and enhancing view modalities available i.e. narrow band imaging (NBI) for Olympus scopes or Blue Light Imaging (BLI) for Fuji scopes.

A thorough endoscopic inspection examination will provide the initial, approximate assessment including the infiltration depth i.e. beyond mucosa and is imperative to plan the next step. The Paris classification (Image 5), based on earlier Japanese classifications, was developed to allow morphological classification of superficial lesions 7,8 . The NICE (NBI International Colorectal Endoscopic) Classification is based on narrow-band images of colonic polyps. The classification uses staining, vascular patterns, and surface patterns to distinguish between hyperplastic and adenomatous colonic polyps. 9 The Japan NBI Expert Team (JNET), which comprises 38 members specialized in colonoscopy, attempted to establish a new NBI classification system for colorectal tumour diagnosis that would overcome the limitations of the NICE classification system 10 (Image 6).
The Size/Morphology/Site/Access (SMSA) scoring system was developed to predict difficulty in polypectomy based on four polyp characteristics: size (S), morphology (M), site (S) and access (A). The score is expressed as four categories with increasing degree of difficulty 11 .
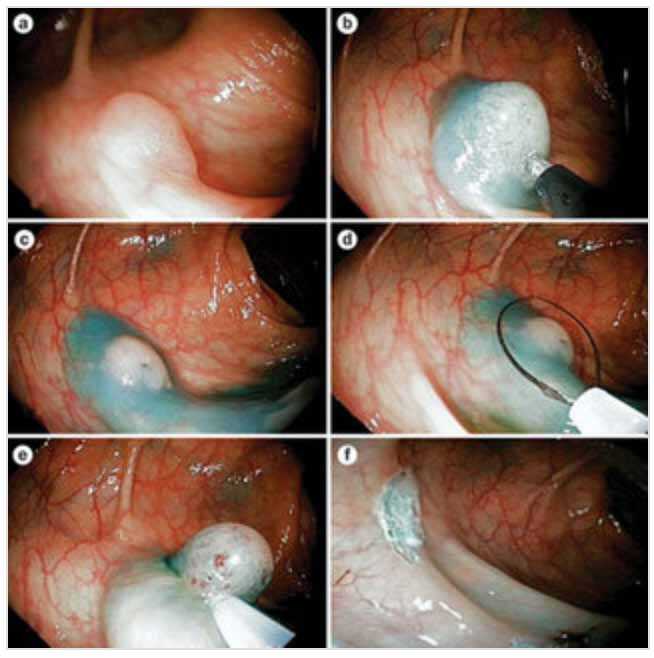
Various polypectomy techniques and devices are available, their use often varying based on local preference and availability 12,13,14 . Endoscopic mucosal resection (EMR) is a technique performed with a polypectomy snare after the lesion has been lifted with a submucosal fluid injection (the “inject-and-cut” technique) (Image 7 & 8). There are other techniques involved i.e. conventional (cEMR) vs underwater (uEMR) EMR, Endoscopic submucosal dissection (ESD), full thickness resection device (FTRD) approach, but, these are beyond the scope of discussion in this article.

En-block resection (full complete resection in one piece) as opposed to piecemeal resection is preferable as the one-piece specimen will enable our Histo-pathologist to determine whether the excision was complete i.e. R0 resection.
Not all lesions are amenable for en-block resection as larger lesions will need to be excised in pieces due to technicality factors mentioned i.e. SMSA scoring system factors.

Main ESGE recommendations 15
- ESGE recommends cold snare polypectomy (CSP) as the preferred technique for removal of diminutive polyps (size ≤ 5mm). This technique has high rates of complete resection, adequate tissue sampling for histology, and low complication rates. (High quality evidence, strong recommendation.)
- ESGE suggests CSP for sessile polyps 6 – 9mm in size because of its superior safety profile, although evidence comparing efficacy with hot snare polypectomy (HSP) is lacking. (Moderate quality evidence, weak recommendation.)
- ESGE suggests HSP (with or without submucosal injection) for removal of sessile polyps 10 – 19 mm in size. In most cases deep thermal injury is a potential risk and thus submucosal injection prior to HSP should be considered. (Low quality evidence, strong recommendation.)
- ESGE recommends HSP for pedunculated polyps. To prevent bleeding in pedunculated colorectal polyps with head ≥ 20 mm or a stalk ≥ 10 mm in diameter, ESGE recommends pre-treatment of the stalk with injection of dilute adrenaline and/ or mechanical haemostasis. (Moderate quality evidence, strong recommendation.)
- ESGE recommends that the goals of endoscopic mucosal resection (EMR) are to achieve a completely snare-resected lesion in the safest minimum number of pieces, with adequate margins and without need for adjunctive ablative techniques. (Low quality evidence, strong recommendation.)
- ESGE recommends careful lesion assessment prior to EMR to identify features suggestive of poor outcome. Features associated with incomplete resection or recurrence include lesion size > 40 mm, ileocecal valve location, prior failed attempts at resection, and size, morphology, site, and access (SMSA) level 4. (Moderate quality evidence; strong recommendation)

Surveillance
Rutter et al. 16 has recently published the updated endorsed BSG/PHE/ACPGBI guidelines (2020) for post polypectomy surveillance. This guideline takes into account the introduction of national bowel cancer screening.
Conclusion
- Colonic polyps involve extensive planning management from the point of pre-intervention with initial diagnostic intention which may convert to therapeutic intervention intra-procedure.
- High quality colonoscopy is a pivotal element for polyp initial detection and subsequent proper management.
- Polypectomy is a high risk endoscopic procedure and proper informed consent pre-procedure is imperative.
References available on request
If you would like to receive an HPN magazine every month, complete the form below to be added to the mailing list. Only those who meet the expected criteria for readership will be added to the list. SUBSCRIBE
Follow us: