

Innovative technology in (AF) Atrial Fibrillation Ablations; A Step to the Future
Background and Scope of problem: Atrial fibrillation (AF) is a common cardiac rhythm disturbance, and its prevalence increases with advancing age. Put simply, AF is an uncoordinated atrial electric activation that results in ineffective atrial contraction and hence reduced stroke volume and subsequently reduced cardiac output. It affects a substantial proportion of the population, approximately 37.5 million people worldwide. In Ireland, AF affects around 11% of adults aged over 65 years and up to 25% at the age over 80 years. It is undeniably a cause of disability, imposing additional burden on the healthcare system.
Reducing Atrial Fibrillation Burden:
The attention, in contemporary medical authorities, has therefore been focused on reducing AF burden through early screening of target groups, diagnosing, treating AF and avoiding its complications thereof – stroke, heart failure and dementia. The range of treatment options include lifestyle changes, such as, increasing physical activity, weight loss, smoking and alcohol avoidance and oral anticoagulation. Rhythm strategy can be achieved by antiarrhythmic drugs, cardioversion and/ or Pulmonary Vein Isolation (PVI) ablation. Guidelines (either European or American) recommend catheter ablation in symptomatic patients who are refractory to drugs, with heart failure and likewise younger group of patients with high exercise endurance.
Rhythm strategy should be discussed between arrhythmia specialists and patients ahead of rate control strategies as the clear benefit in all aspects is quite well established- it improves functional capacity and quality of life, at the same time reducing the long-term risks of stroke, morbidities and hospital admissions in patients with AF. It reduces the need for anti-arrhythmic drugs, which often come with a wide range of side effects, namely thyroid dysfunction or lung fibrosis. In addition, patients with low to moderate stroke risk might be allowed to discontinue blood thinners and hence minimising the accumulated risk of bleeding.
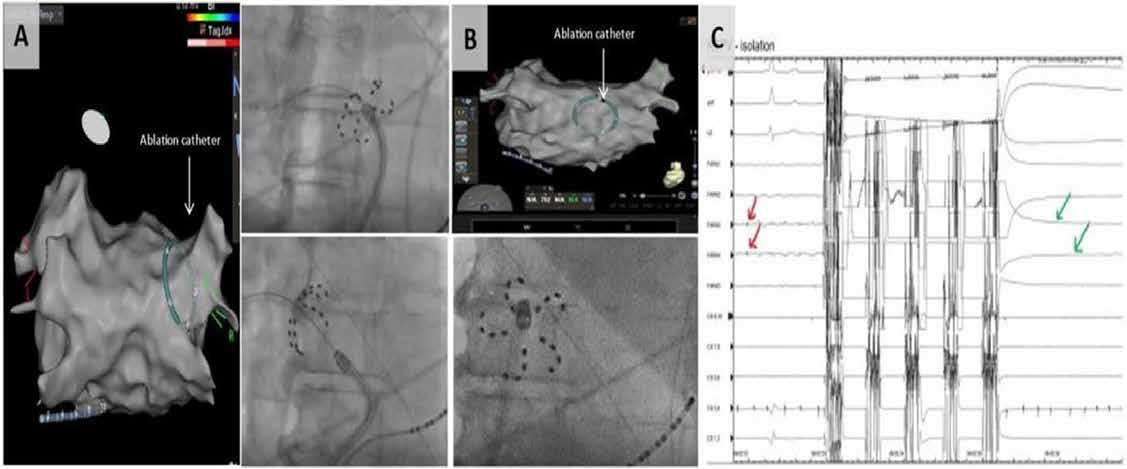
Fig 1: A) PFA multi-electrode catheter in 3 D map around Right Superior Pulmonary Vein on the left panel while Right panel is X Ray of the same configuration. B) Application of PFA on the posterior wall, in some cases with Persistent AF as an additional strategy to the procedures. C) Red arrows show Pulmonary veins potential pre application, then 5 pulses of ablation for 2 seconds at 2000mV and finally green arrows revealed complete resolution and isolation of the pulmonary veins potentials.
Advances in Technology of AF ablation:
The advances made in ablative technology, namely pulsed field ablation and high power with short duration radio-frequency ablations created a paradigm shift in the current management of AF.
A) Pulsed field ablation (PFA):
Is a non-thermal ablative modality that is highly safe as it is tissue selective. Antral application of PFA around the pulmonary vein areas are guided by X-rays and / or 3 D mapping and then energy is transmitted through multi-electrode catheters. Each vein requires 4 applications of 2 seconds each. The scar tissue formed, blocks the electric signals from the veins, thereby isolating the pulmonary veins (Fig. 1). The mechanism of action lies in creating pores within the cell membranes, leading to irreversible apoptosis of the antral endocardial cells- the term called electroporation. Importantly, various tissues have specifically characteristic threshold field strengths that induce necrosis. Myocardiocytes have the lowest threshold values of any tissue. This myocardial sensitivity limits collateral damage of non-target tissue such as the oesophagus and phrenic nerve and hence avoids complications. PFA also spares the extra cellular matrix, preventing disruption of tissue planes and minimises the risk of pulmonary vein stenosis. Recent studies comparing RFA and PVI with PFA confirm superiority in terms of outcome, durability of lesions, as well as safety.

Fig 2: Example of high power – short duration RF of PVI procedure. Dotted red points represent effective RF lesions around the pulmonary veins. Middle of screen, the bale green circle with red circle indicates the accuracy of the catheter tip and contact with endocardial tissue to ensure accuracy to delivery effective RF lesions.
B) High power- Short duration
Radiofrequency ablation:
The conventional approach of using radio-frequency (RF) energy, of a thermal nature, had its own limitations. In recent years, the novelty of high power (90 watts) and short duration (4 seconds) meant that the ablation phase could be reduced to only 5 mins and all procedure time to 25 mins – much reduced from former procedural times of around 180 mins in the near past. This means that more procedures can be performed in the Cath lab and subsequently drive the lower cost of the procedure. Furthermore, the high safety profile of the newer technology would encourage performing it in elderly group of symptomatic patients, who in the past were excluded due to limitations of previous rhythm strategies.
The Future for AF treatment:
Catheter ablation remains a minimally invasive procedure with overall complication risks less than 1%. In clinical practice, however, it is not uncommon to find that the knowledge regarding treatment options, amongst patients with AF, to be suboptimal. There are at times the fear or misconceptions about newer technology, that can be a hindrance. That said, more attention needs to be paid towards improving the perception of emerging technology within the community and clinicians to be better advocate for their patients. Rhythm strategy in AF management must emphasise on the new technology that would reduce complications rate and increase procedure safety, reduce procedure time and hence rapid recovery, reduce cath lab time, increase volume of performed procedures, reduce waiting lists, reduce the overall cost, increase opportunities for training, minimise the related budgets to drugs, hospital admissions and related complications.
The future is ever so promising in this ablation era, with innovative technology unfolding and evidence backed up by valid trials. From low voltage myocardium guided ablation, to epicardial or ganglion ablation, it will take some well-trained Electrophysiologist equipped with the new technology to promote and uplift the current management strategies of AF and maintaining the international standard.